Cell Therapy is Making Progress Against Solid Tumors — But is Anyone Noticing?
Three under-the-radar cell therapy readouts from ASCO 2026 and where the near-term commercial future for this class may lie

Traditional autologous ex vivo cell therapy has largely fallen out of favor. Attention (and dollars) are far more focused on in vivo approaches that massively condense the cost, speed, and complexity associated with the cell therapy supply chain.
The early data from this field has been really promising. At ASCO, Kelonia (newly acquired by Lilly LLY 0.00%↑ ) continued to show a 100% overall response rate (ORR) in multiple myeloma, with more patients and longer follow-up. Just recently, at EHA, Legend Biotech LEGN 0.00%↑ also showed a 100% ORR with 83% complete response (CR) rate in patients with Non-Hodgkin’s lymphomas. And not too long before that, CREATE Biomedicines raised $122M in funding to take more of their programs into the clinic.
Most of the big newsy readouts coming out of ASCO this year were also from outside traditional cell therapy, with it feeling like targeted therapy approaches (whether they be small molecule, ADCs, or otherwise), were stealing the show, and that is justified.
But amidst all the focus on other areas, ASCO did bear some meaningful, albeit iterative, progress against solid tumors. Here are three updates that caught my attention and speak to the iterative progress cell therapy is making in treating solid tumors.
If you subscribe to Big Pharma Sharma (BPS) for my free weekly Last Week Tonight in Biopharma news series and you like what you read there, please consider upgrading to paid to read my best work.
I recently did a deep dive into two interesting data readouts from ASCO 2026 in Lung Cancer. I compared Summit’s ivonescimab to Merck/Kelun’s Sac-TMT and gave you my take on who looks to be the better drug thus far.
You can check that out by following the link below

1️⃣ Obsidian’s OBX-115 Posts 67% ORR in Post-Checkpoint Melanoma With No IL-2, Outpatient Lymphodepletion, and an Optional Needle Biopsy
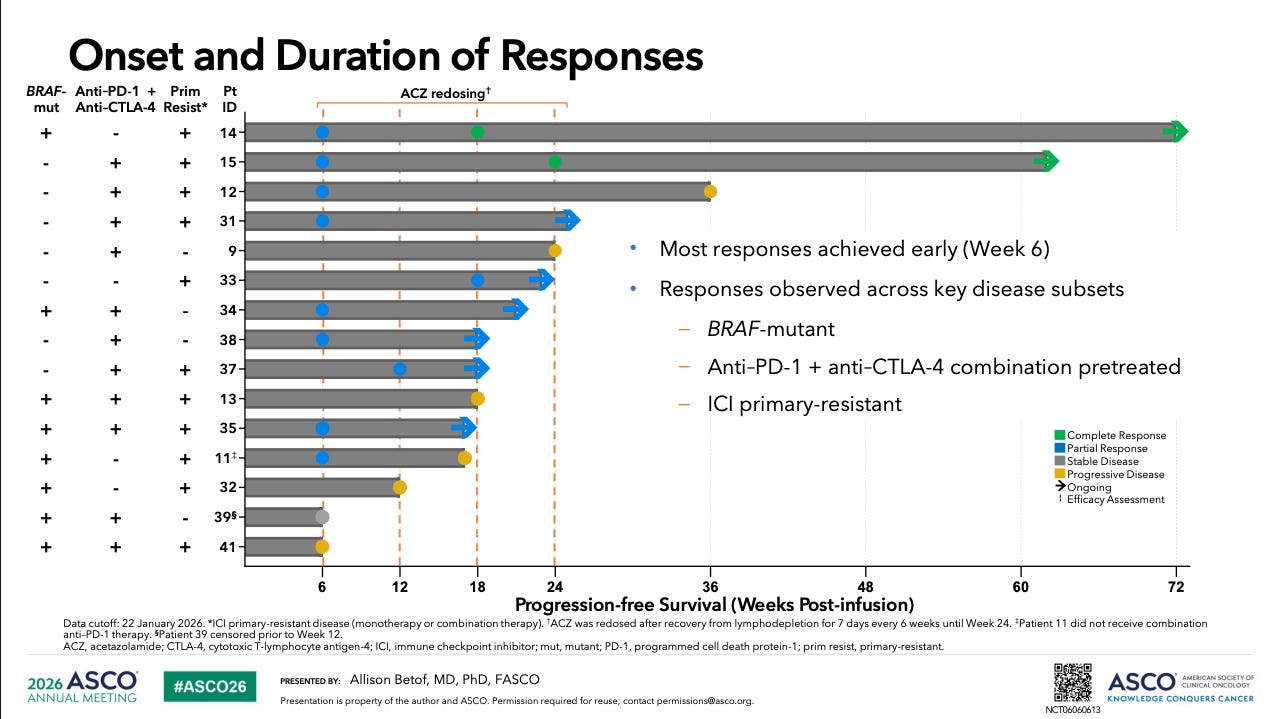
Obsidian presented updated RP2D data for OBX-115 in advanced melanoma that progressed on or after checkpoint inhibitor therapy.
In 15 patients treated at DL3/RP2D (100 × 10⁹ cell maximum), OBX-115 delivered a 67% ORR (13% CR) (10/15; 2 CRs, 8 PRs), a 93% DCR, and tumor burden reduction in 83% of patients. Median DOR was not reached (range 1.1+ to 14.9+ months) at a median follow-up of 4.3 months. Responses were observed across the hardest disease subsets: 73% had prior anti–PD-1 plus anti–CTLA-4 combination exposure, 53% were ICI primary-resistant, and the cohort included BRAF-mutant, mucosal, and acral subtypes.
Safety differentiation showed up too: exclusively low-dose lymphodepletion (Cy 750 mg/m² × 3, Flu 30 mg/m² × 4), no IL-2 in the regimen, CRS in 33% with one Grade 3 event, no DLTs, no ICANS, no ICU transfers, no treatment-related mortality, and 100% of acetazolamide re-dosing handled in the outpatient setting.
Tumor tissue procurement was feasible via core needle biopsy in 2 of 15 patients (both responded). ctDNA dropped by Day 14 in all responders, with 3 clearing entirely.
What I appreciate about OBX-115 is that it is an asset that is intentionally designed to address many of the major bottlenecks that have held first-generation TIL therapies, namely Iovance’s IOVA 0.00%↑ AMTAGVI (lifileucel), back from major market adoption. AMTAGVI’s launch has been constrained by the regimen itself: high-dose IL-2 mandates ICU-level monitoring, myeloablative lymphodepletion locks patients into inpatient stays, surgical tumor harvest limits the patient pool to fit patients with accessible lesions, and the time to treatment is still approximately two months long.
OBX-115 offers a solution to most of those barriers. Swapping out IL-2 for its own acetozolamide triggered membrane-bound IL-15 based cytokine support means patients can avoid additional in-patient days post-infusion. It also offers docs the ability to re-trigger IL15 stimulation and help drive more durability response days after cells have been infused. Low-dose lymphodepletion means outpatient-compatible administration. The core needle biopsy offering also adds flexibility to the manufacturing process, offering a less invasive path of cell collection and thus more patient eligibility. However, given this was only feasible in two of fifteen patients in the study, I am less optimistic that this will be a commonly used feature in the real-world setting. Core needle biopsy also gets more challenging as you move into non-skin cancers.
However, if you are an oncologist who has been reluctant to refer patients for AMTAGVI because the regimen is brutal and the logistics are punishing, OBX-115 is the version of TIL therapy you would be more likely to use. AMTAGVI is a good drug for the sub-segment of people who can receive it, and in the thirty-ish percent of patients who end up getting a response, that response tends to be quite durable. So the problem you need to solve is upstream of the treatment. How do you remove barriers to get more people onto therapy? Or how do you more quickly select the patients who will do well on the therapy?
A 67% ORR in 15 patients at 4.3 months of follow-up is not the same readout as AMTAGVI’s 31.4% ORR in the C-144-01 registrational dataset with 36.5-month median DOR, or the 44% real-world ORR Iovance has reported. But it is an early signal that adds more proof to the differentiation case of OBX-115. The engineering that went into its cell design seems to be driving up efficacy. That is likely due to both the higher percentage of CD8 T-cells in the OBX-115 (98%) and the built-in IL-15 stimulation. More longitudinal data is needed, but this is a promising sign that OBX-115 has raised the bar for TIL efficacy in a post-PD-1 setting.
The trade-offs and remaining challenges of this approach are clear as well though. Adding IL-15 to the mix adds cytokine release syndrome (CRS) back on the table as an on-target AE. TILs on their own don’t generate CRS or neurotoxicity/ICANS, since they’re just natural unmodified T-cells. Obsidian has also done nothing in this iteration to solve the major manufacturing challenges associated with TILs. This is conceivably still a product that takes 1-month plus to manufacture, especially if you’re dosing this at 83B cells. You can’t really speed up cell division more than it already is in an ex vivo centralized manufacturing process, where T-cells are getting every flavor of biological accelerator in the bioreactor.
Still, this is at least a few steps in the right direction, and should serve as a welcome addition to the melanoma armamentarium if/when this is approved. Nothing really works in melanoma after you fail PD-1 based therapy other than AMTAGVI, but not enough people are eligible to receive it. Obsidian’s next readout is expected to be in lung cancer in 1H 2027.
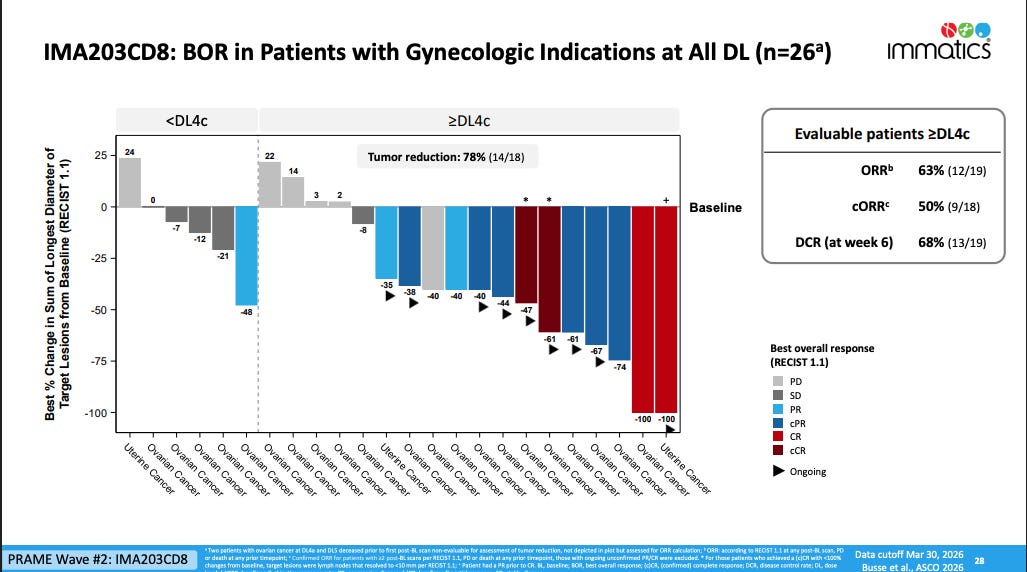
2️⃣ Immatics’ IMA203CD8 Posts 63% ORR in Heavily Pretreated Gynecologic Cancers at ASCO 2026